A pristine office with a stocked bookshelf and framed diplomas on the wall. In an armchair, a therapist sits, making a quick scribble on a notepad. Across a long couch lies a patient, arms crossed and eyes wandering up to the ceiling. The clock hits 50 minutes. As the two depart on their way, the office door closes. On one side, the patient breathes a sigh of relief. This is a scene portrayed many times before, but what happens on the other side of the door?
For psychotherapist Wendy, the door closes, and she has 10 minutes — just enough to run to the bathroom quickly, before her next client — one of five to seven she will see that day. Wendy requested to be identified only by her first name to protect her patients’ privacy.
For Associate Director of Clinical Training at the University of Southern California Clinical Psychology program Dr. Brittany Beasley, her sessions are with graduate students. One of her many roles is as a clinical supervisor.
After the door closes and the patient leaves, a therapist trainee is required to complete extensive clinical supervision. A supervisor is a licensed practitioner who reviews graduate students’ or associates’ patient cases and notes to ensure their work meets ethical standards. Some programs also require students to participate in weekly personal therapy sessions.
This therapist-to-supervisor relationship is comically or dramatically depicted in media, showing the moments on the other side of the door, whether that is Jimmy Laird and Dr. Paul Rhoades in “Shrinking” or Dr. Jennifer Melfi and Dr. Elliot Kupferberg in “The Sopranos.”
In practice, the therapist-to-supervisor relationship often lends itself to guidance and support in a profession that can take a heavy personal toll. In this profession, therapists learn to cope with the multiple facets of the human experience. While none of the sources could give specific details because of patient confidentiality, one could imagine challenging daily confrontations with death, abuse, violence, trauma and grief.
Conversations with the individuals who understand different areas of this issue gave a sense of just how personal the experience is.
After a particularly difficult case in her early career, Wendy cried the whole weekend.
“I heard like seven traumas a day. You hear it over and over and over again, so you do habituate to it. But whoa, it is just the most heinous stuff that’s ever happened to people, and it’s a lot to hold,” she said.
At her first trainee site, Wendy worked primarily with homeless women on domestic violence cases. The site did not provide any one-on-one supervision. Instead, they participated in group supervision where the licensed clinician often deferred to other people in the room to answer each other’s questions. She described it as an unsupportive environment.
However, Wendy’s next job was an entirely different story. To earn hours toward her license, Wendy worked with Veteran Affairs for free. There, she was paired with a supervisor who supported her own professional development and the care of their clients.
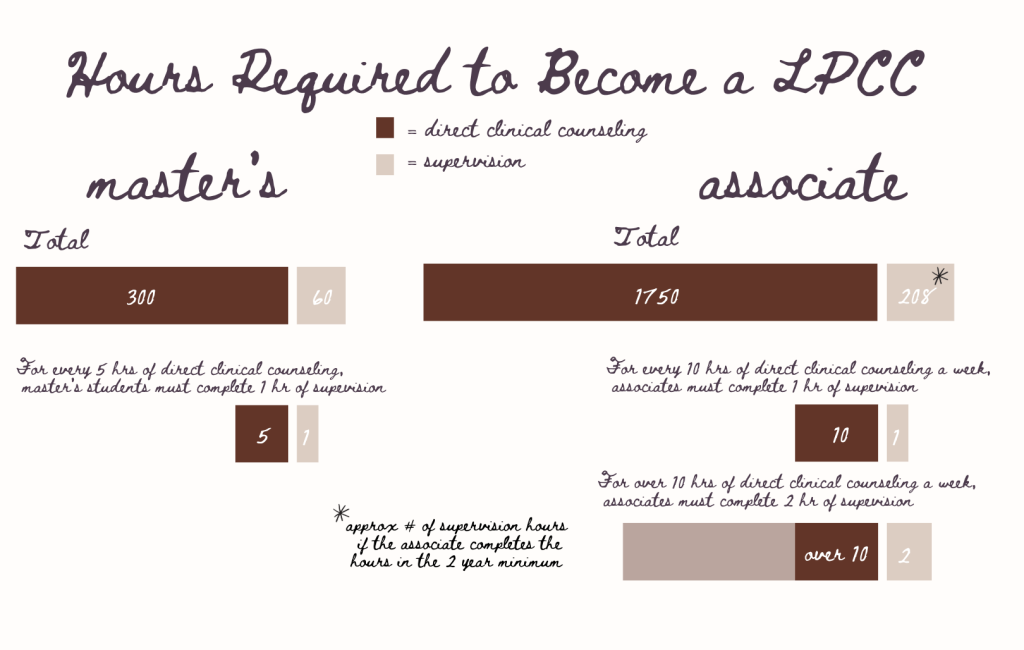
To become a licensed therapist or LPCC, therapists must complete a two-to-three-year-long MMFT or MMHC master’s program. After their master’s, students will become an associate or APCC for a minimum of two years and up to six years. During both the master’s and associate roles, trainees will complete directing counseling hours with patients and supervisions.
Now 20 years into the profession, Wendy regularly works on PTSD and trauma with veterans. Since those early years, Wendy has never again needed an all-weekend cry. However, despite becoming acclimated to such difficult work, she has found it critical not to become jaded.
She attributes the most important thing to being emotionally present with the client. “I have remained committed to not turning my heart off because I have seen clinicians who do that,” she said. However, she also explains that this profession requires personal self-care.
For Wendy, there is not much time between sessions to implement this practice. Now, she unwinds by swimming in the ocean with her friends, going for a walk, or experiencing nature. To prepare for the day ahead, Wendy has developed a morning ritual at the recommendation of several friends.
Driving home from work has become a time she meets with intention around the media she consumes. “My tendency is to be a little too addicted to the news and getting spun up about political stuff, and so that really has not been beneficial for my mental health and certainly doesn’t help me after a full day of seeing clients,” she said.
After more than two decades in the field, she recommends that trainees entering the field find a similar way to replenish their battery, get time to themselves, and go to personal therapy.
Often, stigmas or guilt surround a practitioner’s struggles with the challenges of the psychology profession. On the contrary, Beasley sees these reactions as a cue to a therapist’s “humanness.”
“We are not robots in the room. We are people in the room. And so are there ways where, if we are having experience, we lean into it in terms of empathy,” she said. “Is this showing an empathic response? Is there something very empathic I could say in this moment that reflects my true humanness?”
Now, Beasley will use this empathetic response in session to tell the client how it has impacted her. “I will say, ‘Wow, when you said that, that really hit me. I’m feeling it right here. I’m wondering how you’re feeling?”
In Beasley’s career, there have been moments where she’s felt her guilt creep in. “I can recall times when I was early in practice, where it felt very vulnerable to say, ‘This is heavy,’ because it felt like I couldn’t handle it,” she said. “I think if we can let go of that, ‘I can’t handle it,’ to ‘Hey, I’m human, and this is heavy, and I would love a space to be able to unload it and talk to someone else.’ Then, that also provides a rich opportunity.”
Now, Beasley uses her expertise to guide other students through their entry into the field as an associate professor and clinical supervisor at USC’s Clinical Psychology program.
Students working at the departmental clinic provide therapy to USC students, faculty, staff and individuals in the community. As a training clinic, clients consent to recorded sessions. During weekly one-on-one supervision, Beasley watches the clinical recordings and provides feedback on treatment plans and interventions.
In her supervision session, Beasley prioritizes validating her students’ experiences. She explains that, as a culture, we tend to minimize how validation can bring down distress. “Sometimes, we hear very challenging stories. Sometimes, we’re trying to figure out how do we not take that home with us. How does that not impact our emotional well-being?” she said.
She also emphasizes self-awareness of one’s own triggers when often students are surprised by the triggers or reactions that can arise during a session. “Sometimes we’re in our own heads because of having reactions, then we can kind of drift off. How do you gently and compassionately let your mind say, ‘Hey, I’m having that reaction. I’ll get to that later?’ [How do I] bring myself back to the person who’s in front of me and stay present with them,” said Beasley.
Beasley says it is also critical that students find support after a difficult session. Being mindful of psychology’s strict ethics around client confidentiality, students can process their work with clinic supervisors or peers.
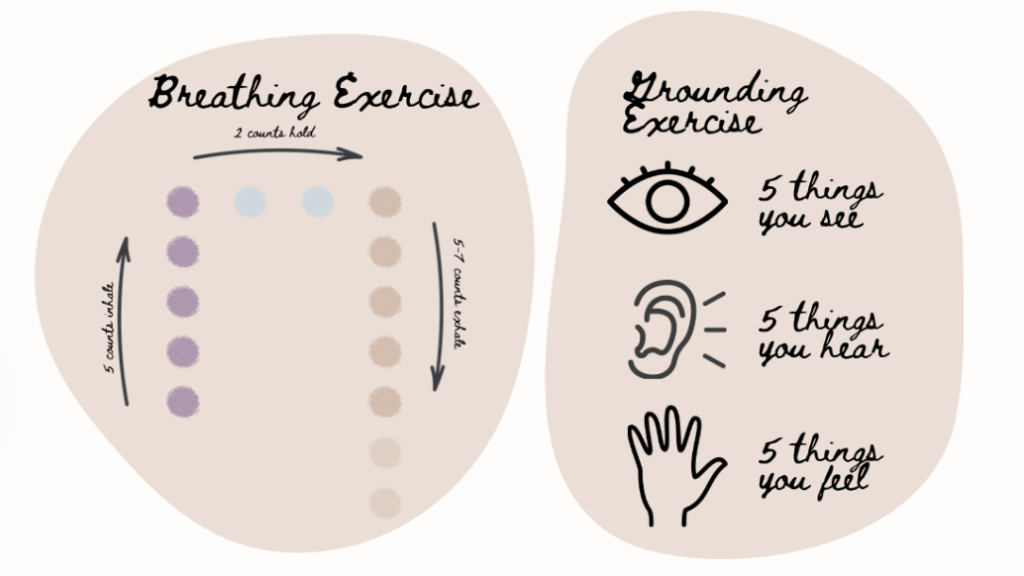
Beasley also recommends that students practice breathing, grounding, compassion, and self-reflection exercises after work and meet with their own therapists.
In class, Beasley provides an opportunity for students to talk through their struggles together. Her students compare stories and co-create options for each other. In their first semester, students will take Beasley’s professional issues class, which identifies signs of burnout.
In her coursework, Beasley has also utilized Jeffrey A. Kottler’s “The Therapist Workbook.” This workbook discusses the “consequences of this choice” as students complete worksheets reflecting on their expectations, hopes and personal motives.
In an exchange with Kottler, he explained that therapists sometimes experience countertransference, which is an emotional response to the client based on a therapist’s own personal history. “Most therapists learn to enforce boundaries so they don’t overreact personally to the trauma and troubles,” he explained.
A seasoned professional and author of more than 120 non-fiction books, Kottler said that over the years “I’ve learned to allow myself to feel my clients’ suffering as part of empathy.”
USC Assistant Professor of Clinical Psychology Dr. Bruna Martins-Klein brings conversations like those in Beasley’s class into her non-psychology classes. In her courses, she prioritizes small discussions. “This gives them the opportunity to each take turns being a speaker versus listener and engage in empathic listening,” said Martins-Klein. In this exercise, listeners repeat what they understood from the speaker, and the speaker provides corrective feedback.
In her own work, Beasley focuses on the human element. “I think it is quite an honor to be able to be on the journey with someone as they grapple with human experiences and with life and with any other mental health challenges or supports they might be facing,” she said. “I think it is really important and shouldn’t be taken for granted that when you’re sitting side by side with someone sometimes through some of the hardest moments of their life, it can be a challenge on how do you not only do that in the moment but sit with that and grapple with that afterward?”
To protect the privacy of their patients, some therapists couldn’t participate in a written interview. While we can’t see their faces or read their names, audio allows us to hear their unique perspectives on the challenges and positives of the profession.
Conversations with therapists on and off the record revealed that even though this profession can be taxing, they love it. The words that kept coming up to describe their patients were “heroes” or “warriors.”
“I wouldn’t ever want another job. I like the intensity of it. I like walking with people through this,” said Wendy. “I feel like they’re warriors, being willing to walk through this pain to get to the other side and it’s a total honor to do that with them.”
Former emergency room psychologist Robert experienced the dichotomy of this work to an extreme. He was faced with death every single day. However, Robert considers himself lucky to have been confronted with it. “Our society doesn’t like dealing with death. Everyone has to see that stuff, and we’re lucky because we have to deal with it. And if it doesn’t bother you, you probably shouldn’t be in that work,” he said. Robert requested to be identified only by his first name to protect his patients’ privacy.
While working in Haiti after the 2010 earthquake, a doctor told him words that he has held onto throughout his profession: “Sometimes all we can be is a human witness,” Robert explained.
“Everyone wants their story told. Everyone wants a witness to their life. I mean, for egocentric reasons, but that, ‘I am here. I am alive,’ right,” he said. “And sometimes that’s all we can do, and I try to do that.”